Clinicians are trained to act on numbers: BMI, HbA1c, LDL cholesterol. Yet many patients who fall within acceptable ranges already carry early metabolic dysfunction that these markers do not fully capture. The question is where to look earlier.
One emerging site is skeletal muscle.
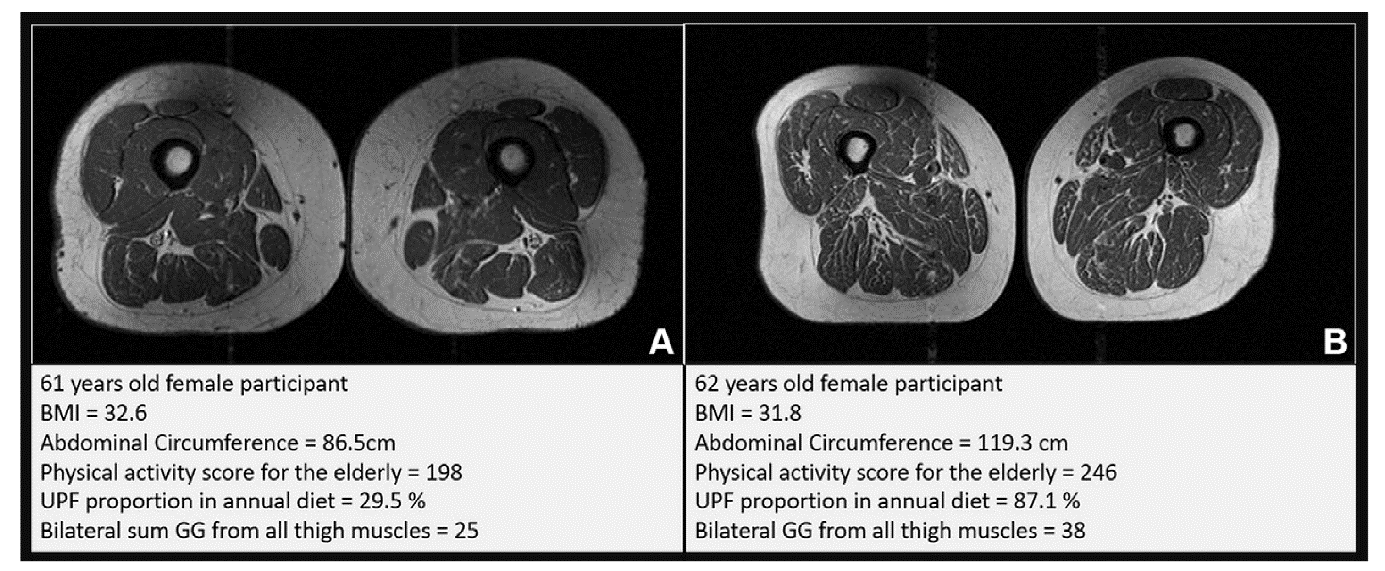
In a cohort of adults at risk for knee osteoarthritis but without overt disease, higher intake of ultra-processed foods was associated with greater fat infiltration within thigh muscle on MRI. The effect was consistent across muscle groups and independent of age, physical activity, and total caloric intake. When central adiposity was accounted for using abdominal circumference, the association strengthened, suggesting that distribution of fat, not just total mass, is clinically relevant.
This matters because skeletal muscle is a central metabolic organ. It accounts for a large proportion of postprandial glucose disposal. When fat accumulates within muscle fibers, insulin signaling becomes less efficient, oxidative capacity may decline, and local inflammatory signaling increases. These processes precede and predict insulin resistance. In other words, the tissue is changing before the laboratory values do.
The study is cross-sectional and cannot establish causality. Dietary intake was self-reported, and classification of ultra-processed foods is imperfect. But the direction is biologically coherent and aligns with broader cardiometabolic evidence: diets high in ultra-processed foods are energy dense, protein diluted, and micronutrient sparse, conditions that favor ectopic fat deposition.
From a clinical standpoint, this reframes diet from a general lifestyle factor to a targeted exposure with measurable tissue-level consequences.
What can be done now in practice?
1. Screen diet structure, not just calories
A brief, focused history is sufficient:
• Proportion of ready-to-eat packaged foods
• Frequency of processed snacks, sweetened beverages, and industrial meals
• Reliance on whole-food meals prepared from basic ingredients
A practical threshold: if more than one-third to one-half of daily intake is ultra-processed, the patient is likely in a higher-risk exposure category.
2. Use simple anthropometric signals earlier.
Abdominal circumference provides more actionable information than BMI in this context. An increase in waist size, even with stable weight, should prompt dietary reassessment and intervention.
3. Act before glycemic markers shift
Do not wait for elevated HbA1c or fasting glucose. Patients with normal laboratory values but high ultra-processed food intake and increasing central adiposity are appropriate candidates for early intervention.
4. Target composition, not restriction alone
The intervention is not simply caloric reduction. It is structural substitution:
• Replace ultra-processed items with minimally processed foods
• Ensure adequate protein intake to support muscle maintenance
• Increase fiber and micronutrient density
This shifts the metabolic environment away from fat storage within muscle.
5. Monitor functional proxies
Changes in gait speed, muscle strength, or fatigue may reflect underlying tissue quality. These are low-cost, clinically accessible indicators that complement laboratory data.
6. Set realistic clinical endpoints
Short-term success is not only weight loss. It includes stabilization or reduction in waist circumference, improved energy levels, and maintenance of muscle function.
What remains uncertain
The current evidence does not prove that reducing ultra-processed food intake will reverse intramuscular fat infiltration. Longitudinal studies are needed to establish causality and reversibility.
However, waiting for definitive proof before acting would ignore a consistent and plausible signal across multiple domains of evidence.
Take away
Ultra-processed food exposure can be treated as an early, modifiable determinant of metabolic tissue quality. Intramuscular fat infiltration is a plausible intermediate phenotype linking diet to insulin resistance and functional decline.
In practice, this supports a shift from reactive management of established cardiometabolic disease to earlier, diet-focused intervention aimed at preserving tissue integrity before dysfunction becomes clinically overt.
Source: https://pubs.rsna.org/doi/10.1148/radiol.251129

